
Examination methods

Basis
In order to tread the person concerned with consideration - as valid to all medical science – there should not be a full diagnosis at the beginning, but rather a step by step escalating examination procedure. Furthermore, the principle of all examinations validates that the diagnosis also should lead to therapy and is not executed as a means of itself.(www.dzz.de/beitragpdf/pdf_1309.pdf).
The examinations should also adhere sensibly, practically and performable to the principle. Provision of the diagnosis of CMD – as advised in all medical science – is an extensive medical consultation with thorough anamnesis. There should be a standardised questionnaire or – schemata as well as a psychological pain questionnaire on regular basis for early detection of psychosocial impairment.
The basis is a “normal” dental examination with identification and inspection of teeth, their fillings, crowns and dentures. Included is the search for decay, a vitality check (mostly known as “cold test”) and PSI (Parodontitis Screening Index) test to identify parodontitis.
A mandatory part is also a x-ray of the whole jaw region (panoramic radiograph) in order to exclude dental and/or a dental operative cause of disease (e. g. displaced teeth, chronic infections of teeth roots, hidden decay or bone deterioration caused by parodontitis).
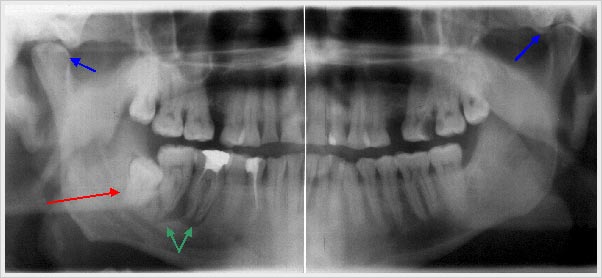 Panoramic radiograph
with displaced tooth (tooth 48 = right wisdom tooth) -red arrow-
Panoramic radiograph
with displaced tooth (tooth 48 = right wisdom tooth) -red arrow-of chronic apicale parodontitis of teeth 46 and 47 -green arrows-
and also an indication of differences in jaw joints -blue arrows-
If the suspicion substantiates, then further dental examinations are necessary: Instrumental model analyses with occlusion and myocentric bite analyses and articulator programming. The articulator consists of a chewing and jaw movement simulator and allows the specialist to detect which factors disturb the bite. If applicable, a MRT (magnet resonant tomopraph) of the jaw joints will show evidence. Other specializations should be consulted in case of complex disease patterns e.g. exclusion of neoplasm – most likely the concerned person has been to possible specialists and are detached from differential diagnosises.
Summary
The specialized dental examination is completed according to “triple A” scheme (acc. to the German terms):
- Listening and questioning
- Scanning by fingertips and touching
- Measuring and calculating
References for standard examination for further interest:
Advantage: Clearly structured result, main emphasis on joint result.
Disadvantage: Musculare result could be more extensive.
CMD-test according to Ahlers (www.prodente.de/test-und-checklisten/cmd-test.html)
Formblätter: www.dentaconcept.de/Formblaetter/Basis-Set.shtml
Advantage: Clearly structured result, extensive transfer questionaire for consulting specialists.
Disadvantage: Muscular result could be more extensive.
RDC-Test (ubwp.buffalo.edu/rdc-tmdinternational/wp-content/uploads/sites/58/2017/01/RDC-German.pdf)
Advantage: The applied strength of examining fingers is too weak in order to get a reaction of most CMD patients. (CMD-patients often do not recognize slight pain signals during examination, because they have experienced pain for years); Muscular results fall short.
Model analysis:
Conclusions can be made from atypical chewing areas and other surfaces of the teeth for possible dysfunctions. However, minimum prerequisite is the arbitrary practiced articulation of the model (meaning: using a so called orthodontic headgear, the model is approaching the jaw joint axle to be set in articulation).Advantage: Easy performance
Disadvantage: The position of the jaw is only recorded in its habitual biting position.
Recording of the joint course:
The movement of the jaw and its joints is recorded while using appropriate electronical aids.Advantage: Reproduceable to the greatest possible extend, the designated joint axle is at most times readjustable, positive diagnostical information, very suitable for documentation
Disadvantage: Very elaborate, does not indicate any reference directly to the therapy or respectively to the therapeutic situation of the bite. Does not determine the correct dental occlusion.
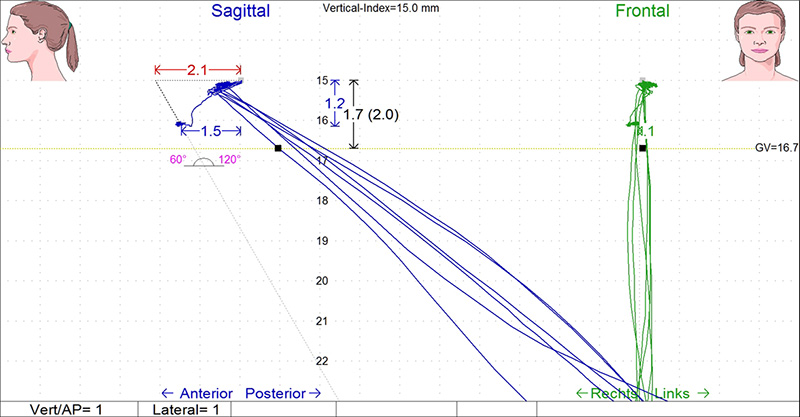
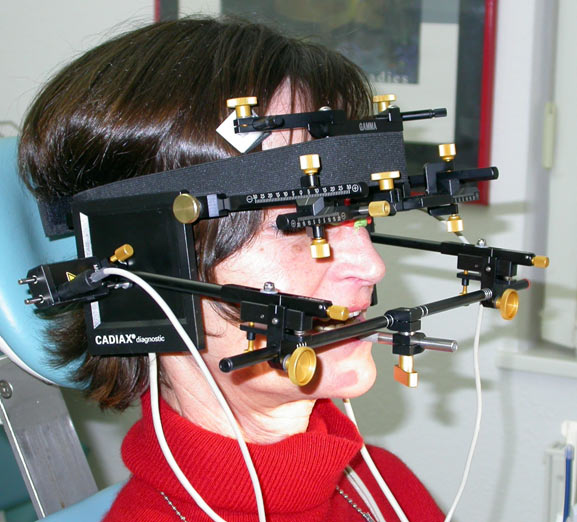 Image of a recording of the joint course and determination of the individual joint axle with the present Cadiax®-System
Image of a recording of the joint course and determination of the individual joint axle with the present Cadiax®-SystemAttention:
The application of the headgear alone does not represent a diagnosis of functions, but rather displays a rough estimation of the relative vertical position of joint axle to the upper jaw!
 Image of arbitrary transmission of the relative vertical position of the joint axle to the upper jaw using the Artex®-headgear and Leipziger Glabellastütze®..
Image of arbitrary transmission of the relative vertical position of the joint axle to the upper jaw using the Artex®-headgear and Leipziger Glabellastütze®..
 A simple articulator offers the best display of mounting the upper jaw into the appliance.
A simple articulator offers the best display of mounting the upper jaw into the appliance.
Identification of dental occlusion:
ManualThis is the best reproduced dental occlusion, since it pushes the lower jaw joint (e. g. Dawson grab) to the upper bone margin of the joint cavern (dorso-cranial position). However, this is not a physiological position (these joint surfaces are most often the infected joint parts caused by overstressing) but is determined through treatment.
Advantage: Reproduceable.
Disadvantage: Results in a pathological vertical position of the jaws to each other.
Habitual
Reflects the present – often pathological – position of the jaws to each other and is in most cases reproduceable.
Advantage: Easy to determine, mostly reproduceable.(www.ncbi.nlm.nih.gov/pubmed/10632846?dopt=Citation)
Disadvantage: Reflects the present pathological position of the jaws to each other.
Myofunctional
The desired jaw relation is represented with elaborate examination technology and can compare the IS-Position due to the position of teeth.
Advantage: Properly reproduceable, the ascertained difference of dental occlusion and muscle manipulated desired position of the jaws is balanced and CMD can be treated successfully.
Disadvantage: Elaborate.
Possible examination methods:
Pen brace
www.ipr-original.de
www.ncbi.nlm.nih.gov/pubmed/11757325?dopt=Citation
www.ncbi.nlm.nih.gov/pubmed/19089144...
 Pen brace
Pen braceThis procedure was introduced in 1905 by Gysi and further developed from McCrane. It is based on the principle, that a 3 point bracing always remains stable and safe and not to be wiggled (e. g. a table with three legs never wiggles).
The dental implementation braces are both jaw joints and a temporary inserted writing pen, which is resting on a writing pad, so that the teeth do not touch each other.
The movement of the lower jaw is recorded in this manner and the muscle manipulated lower jaw position independent of teeth, can be determined.
Advantage: Relatively easy and safe.
Disadvantage: The distance of the jaws to each other must be increased while measuring, so many times until the movement of the lower jaw transfers from the rotation movement into the gliding movement.
The recording is very small without EDP aid.
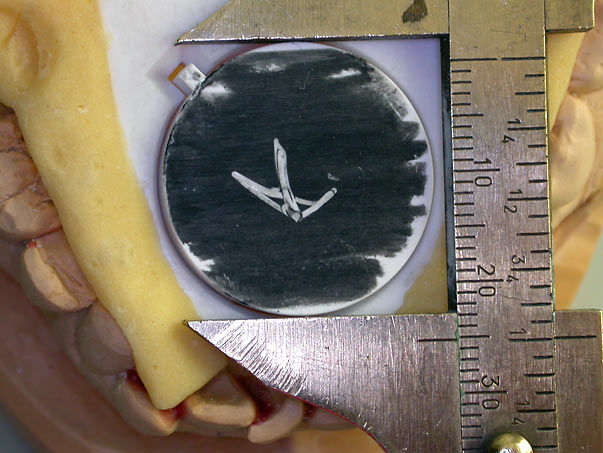 Image of a recording with pen brace in original size
Image of a recording with pen brace in original size(notice sliding caliper as size comparison)
Resource: Vogel further developed the recording of the pen brace with the aid of electronical sensors and initiated a force control simultaneously.
He found out that by inducing force between 10N and 30N on the writing pen, the chewing muscles right and left (rather) tense up; the equal and a lateral crooked pulling of the lower jaw is avoided.
(www.ipr-original.de)
 Patient with EMG electrodes and manibular scanner
Patient with EMG electrodes and manibular scannerEMG:
Electromyography was introduced to dentistry by Dr. Jankelson. The appropriate technology is the K7 evaluation system supplied by the American company Myotronics. The electromyography records the neuromuscular activity of different muscle pairs of the chewing muscles in ease while opening and closing.
The disposition of the muscle controlled occlusion is made possible after the pre-treatment of a low frequency stimulation current via muscle activity.
The analysis of innervation with maximum bite serves the evaluation of occlusion quality of the present situation and at a later measurement, the accuracy of the occlusal splint, respectively the restoration.
Advantage: Very accurate observance of muscle tension
Disadvantage: Very elaborate in appliances; difficult evaluation of occlusion
 With this data from scan 5 the dentist can determine the optimal bite position.
With this data from scan 5 the dentist can determine the optimal bite position.
Further information: www.myotronics.com/products/k7-evaluation-system